


Your Guide To Understanding Back and Leg Pain

Dealing with pain that begins in your back and travels down your leg is a common and deeply frustrating experience. Searching for answers online often leads to conflicting advice, leaving you more confused than when you started.
This article is designed to provide clarity. It explains the framework healthcare professionals use to understand these connected symptoms, helping you make sense of what might be happening in your body.
The Confusing Link Between Back and Leg Pain
It can be difficult to determine if the source of the problem is the back, the hip, or the leg itself. The purpose of this guide is not to provide a diagnosis, but to offer a clearer understanding of the potential mechanisms at play.
When you can articulate your symptoms in a way that aligns with clinical reasoning, conversations with your doctor or physiotherapist tend to become more productive.
Why Are These Symptoms So Often Paired Together?
The connection between back and leg pain can seem puzzling, but from a clinical standpoint, it is a very common pattern. A useful starting point is to understand what sciatica feels like, as this type of radiating nerve pain is a classic example.
The underlying issue is widespread. In England alone, it's estimated that around 1 in 6 people (16.9% of the population) are affected by back pain at any given time.
This prevalence underscores the importance of having access to clear, reliable information.
Identifying the Source of the Problem
When a healthcare professional assesses these symptoms, their initial goal is to determine which of a few primary scenarios is occurring:
-
Nerve Compression: Is a structure in your spine—such as a herniated disc or bone spur—placing physical pressure on a nerve root? Since these nerves extend into your legs, irritation at the source can cause pain, numbness, or tingling sensations far down the limb.
-
Referred Pain: The problem may originate in a muscle or joint in the lower back or pelvis. Even without direct nerve compression, an injury or strain can generate a dull, achy pain signal that is perceived in the buttock or thigh. The brain sometimes misinterprets the origin of the signal.
-
Two Separate Issues: It is also possible that two unrelated problems are occurring simultaneously. For example, a person might have a simple back strain and a separate issue in their hip, knee, or leg muscles.
This diagnostic process forms the basis of any effective treatment plan. It guides the questions you will be asked and any physical tests that are performed.
Why a Back Problem Can Cause Leg Pain
It may seem counterintuitive that an issue in your lower back can produce symptoms down in your leg, but it aligns with the body's neural anatomy. The nerves exiting your lower spine are like major electrical cables branching out from a central hub. These cables run down through the buttocks and into the legs, transmitting signals for both sensation and movement.
If there is an issue at the source—a form of 'irritation' in the spine—the disruptive signals can travel along the entire length of that cable. As a result, the pain, tingling, or weakness felt in your calf may not be a leg problem at all. It is often a direct consequence of an event occurring further up the chain in your lower back.
The Nerves Tell the Story
In a clinical setting, one of the first steps is to determine if the pain follows a specific nerve pathway. This helps distinguish between two different types of pain.
-
Radicular Pain: This is classic nerve-root pain. It is caused when a nerve is directly compressed or irritated as it exits the spine. Patients often describe it as a sharp, shooting, or electric-shock sensation that travels down the leg in a defined line. Sciatica is the most well-known example.
-
Referred Pain: This tends to feel different. It is typically a duller, deeper, and more diffuse ache that is harder to pinpoint. It occurs when a problem in a spinal joint, muscle, or disc sends pain signals that the brain misinterprets as originating from the leg.
This distinction is a critical clue. Radicular pain points towards a potential nerve compression issue, whereas referred pain often suggests a more general musculoskeletal strain or joint problem in the back.
Common Triggers for Nerve Irritation
Several common conditions can cause this nerve irritation.
The most frequent is a herniated disc. The soft, gel-like centre of a spinal disc can bulge or leak out, pressing directly on an adjacent nerve root. For a more detailed explanation, our guide on how to manage a herniated disc explores this mechanism further.
Another common cause, particularly with age, is spinal stenosis. This refers to a narrowing of the spinal canal through which the nerves pass. This gradual narrowing can begin to squeeze the nerves, leading to pain, cramping, or a feeling of heaviness in the legs that often worsens with walking.
A characteristic sign of spinal stenosis is that symptoms often improve when leaning forward—for instance, when pushing a shopping trolley. This posture temporarily increases the space in the spinal canal, easing pressure on the nerves.
Understanding these underlying causes helps explain why treatment is often directed at your back, even when your primary complaint is in your leg. The aim is to address the problem at its source to stop the painful signals from being transmitted.
Common Conditions Causing Back and Leg Pain
When a patient presents with both back and leg pain, a clinician considers a specific list of potential conditions. Each condition has a distinct pattern of symptoms, triggers, and relieving factors.
Understanding these patterns can help you articulate your experience more clearly when seeking professional help.
This flowchart provides a visual representation of how a problem in the spine can transmit pain signals down into the leg.
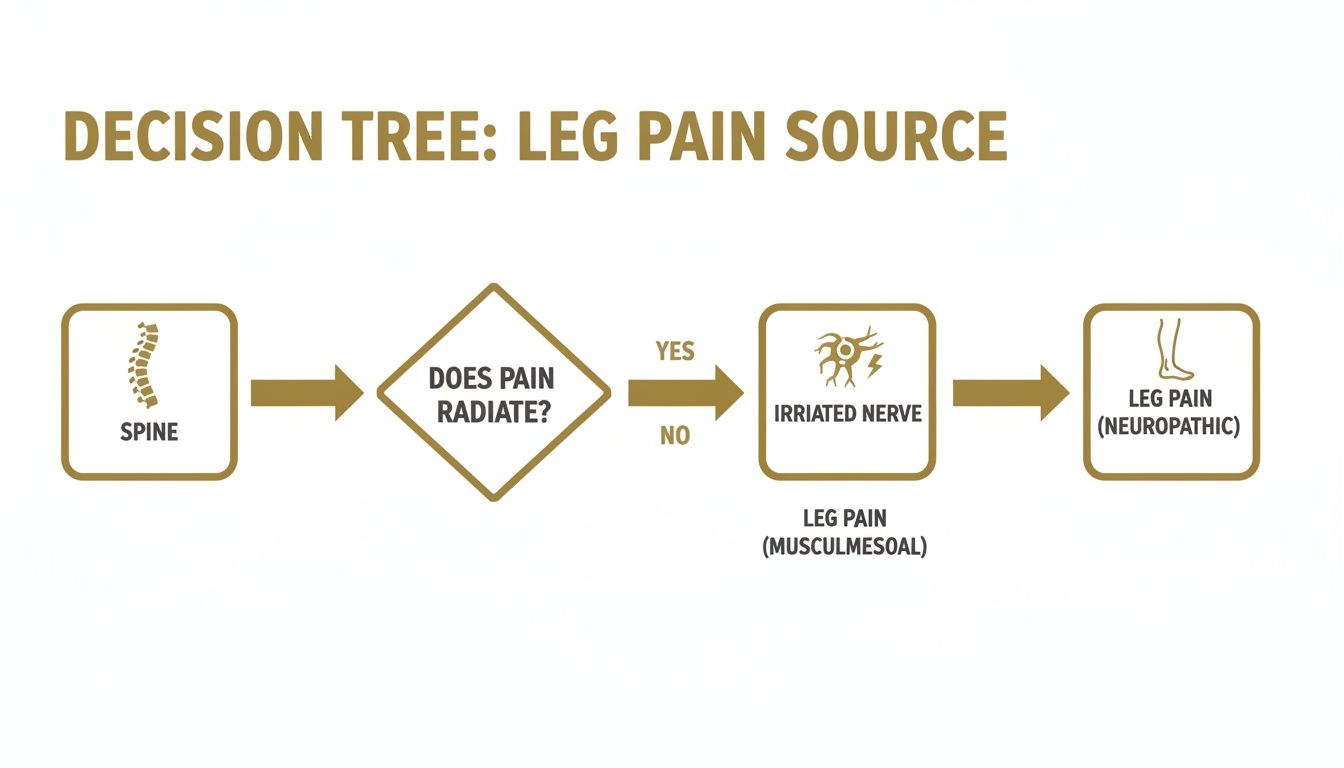
It illustrates the direct pathway from an irritated nerve in the spine to the pain felt in the leg, explaining many instances of radiating symptoms.
Sciatica (Lumbar Radiculopathy)
Sciatica is one of the most widely recognized causes of combined back and leg pain. It is not a diagnosis itself, but rather a symptom indicating that an underlying issue is compressing or irritating the sciatic nerve. This large nerve runs from the lower back, through the buttocks, and down each leg.
The pain is often described as sharp, shooting, or electric, typically affecting only one leg. It can travel from the buttock to the foot and may be accompanied by numbness or tingling. While awaiting a formal diagnosis, learning about Immediate Relief For Sciatica Pain At Home can be helpful.
Spinal Stenosis
The spinal canal is the channel that houses your nerves. In spinal stenosis, this channel narrows, putting pressure on the nerves within. The condition usually develops slowly over many years and is more common in older adults.
The classic symptom is neurogenic claudication—a cramping, aching, or heavy feeling in both legs that worsens with standing or walking. The pain often improves significantly upon sitting down or leaning forward, which provides temporary relief by creating more space for the nerves.
Musculoskeletal and Joint-Related Pain
Not all leg pain originates from a nerve. Sometimes, the problem lies within the muscles or joints connecting the pelvis and spine.
-
Piriformis Syndrome: The piriformis is a small muscle located deep in the buttock. If this muscle becomes tight or spasms, it can compress the sciatic nerve, which runs nearby. This can produce sciatica-like symptoms, typically a deep ache in the buttock that may radiate down the back of the thigh.
-
Sacroiliac (SI) Joint Dysfunction: The SI joints connect the spine to the pelvis. If these joints become inflamed or move improperly, they can cause low back pain that refers a dull, achy sensation into the buttock and sometimes the upper thigh.
-
Lumbar Strain: A simple muscle strain in the lower back can also refer pain elsewhere. While the primary injury is in the back muscles, the pain can spread, causing discomfort in the buttocks or upper legs.
This table summarises the typical characteristics of each condition.
Distinguishing Common Causes of Back and Leg Pain
| Condition | Typical Pain Description | What Makes It Worse | What Makes It Better |
|---|---|---|---|
| Sciatica | Sharp, shooting, "electric" pain, often with numbness/tingling down one leg. | Sitting for long periods, coughing, sneezing. | Lying down, walking (for some). |
| Spinal Stenosis | Aching, cramping, or heavy feeling in both legs. | Walking, standing upright. | Sitting down, leaning forward. |
| Piriformis Syndrome | Deep, dull ache in the buttock, may radiate down the back of the thigh. | Sitting, climbing stairs, running. | Stretching the piriformis, walking. |
| SI Joint Dysfunction | A dull, one-sided ache in the low back, buttock, or upper thigh. | Standing up from sitting, rolling in bed. | Lying down, gentle movement. |
Comparing these patterns reveals important clues. For example, pain that travels past the knee often suggests nerve involvement, while a deep ache that remains higher up is more likely related to a muscle or joint.
Knowing When to Seek Urgent Medical Care
In most cases, back and leg pain can be managed with guidance from a GP or physiotherapist. However, certain symptoms can indicate a condition that requires immediate medical attention. These are known as ‘red flags’.
This information is not intended to cause alarm, but to empower you to act appropriately if a rare but serious situation arises.
The Most Urgent Red Flag: Cauda Equina Syndrome
The most critical condition to be aware of is Cauda Equina Syndrome. It occurs when the bundle of nerves at the base of the spine is severely compressed. This is a surgical emergency where prompt treatment is vital to prevent permanent damage.
Look for this specific combination of symptoms occurring together:
- Bladder or bowel dysfunction. This includes the inability to urinate, loss of the sensation of needing to go, or new-onset incontinence.
- Numbness in the ‘saddle’ area. This is the part of your body that would be in contact with a horse's saddle: the inner thighs, between the legs, buttocks, and genital area.
- Progressive weakness in the legs. This is a significant loss of power that makes it difficult to move your legs or feet properly.
If you develop these symptoms, you must go to the nearest A&E department immediately.
In a clinical context, a patient presenting with this combination of saddle numbness, bladder changes, and significant leg weakness requires immediate action. The sooner it is addressed, the better the potential outcome.
Other Signs That Require Prompt Assessment
Beyond Cauda Equina Syndrome, a few other symptoms warrant a prompt medical evaluation to rule out underlying issues like a spinal infection or fracture.
Seek medical advice if your pain is accompanied by any of the following:
- A fever and feeling generally unwell.
- Unexplained and significant weight loss.
- The pain is severe and relentless. It is constant and not relieved by rest or changing position.
- The pain began immediately following a significant trauma, such as a serious fall or car accident.
These symptoms do not automatically signal a serious problem, but they do require professional evaluation.
How a Specialist Investigates Your Pain
When you consult a professional for back and leg pain, the process begins with a conversation, not a scan. Your description of your symptoms provides the most important initial clues.
This clinical history is the most critical part of the assessment. Your clinician will ask specific questions to build a detailed picture of your condition.
It All Starts with Your Story
The goal is to understand the unique "personality" of your pain. A clinician will likely ask about:
- The Journey: Where does the pain start and where does it travel? Does it stop at the buttock or continue past the knee?
- The Feeling: What is the quality of the pain? Is it a sharp, electric shock? A deep, dull ache? Or a burning or tingling sensation?
- The Triggers: What activities aggravate it? Is it prolonged sitting, standing, walking, or something as simple as coughing?
- The Soothers: Conversely, what provides relief? Does lying flat help? Do you find yourself leaning forward to ease the ache?
- The Timeline: When did it begin? Has it been gradually worsening, or does it come and go?
Detailed answers to these questions help the clinician differentiate between nerve-related pain and pain originating from a muscle, joint, or other structure.
The Hands-On Physical Examination
After listening to your story, a physical examination is performed. This involves a series of tests to assess your movement and neurological function, which helps confirm or refine the initial diagnostic ideas.
This is a structured evaluation, not a random assessment:
- Movement Check: You will be asked to move your spine in various directions—bending forward, backward, and side to side—to observe which movements reproduce your symptoms.
- Nerve Tests: To assess nerve health, your clinician will test your reflexes, check the strength in your leg muscles, and evaluate your sensation to light touch.
- Special Tests: A classic test is the straight leg raise. While you lie on your back, the clinician gently lifts your straight leg. If this action reproduces the nerve pain down your leg, it is a strong indicator of nerve irritation.
In clinical practice, a thorough history and a targeted physical examination provide enough information to form a solid working diagnosis in the vast majority of cases. This is why imaging scans are not typically the first step.
The persistence of these conditions is a significant public health concern. One study suggests men may have a greater risk of recurrent back pain over time, highlighting the importance of a clear diagnosis and a long-term management plan. You can read more in the full research on back pain prevalence.
When is an Imaging Scan Necessary?
It is common to assume that an MRI scan will provide the definitive answer. However, imaging is used more selectively in practice. It is a valuable tool, but it is reserved for specific situations.
Scans are typically considered when:
- "Red flag" symptoms are present that may suggest a more serious underlying condition.
- Symptoms are not improving after a consistent course of conservative treatment, such as physiotherapy.
- The scan results would directly influence the next step in treatment—for example, if surgery is being considered and a surgeon needs a detailed anatomical map.
This careful, step-by-step approach ensures that your treatment is guided by your clinical presentation—your symptoms and functional limitations—not just by an image of your spine.
Your Path to Managing Back and Leg Pain

Understanding the potential cause of your back and leg pain is the first step. The next involves treatment, which clinicians typically approach in layers, beginning with the simplest and safest strategies.
This progressive approach gives your body the best opportunity to heal with minimal intervention.
The Foundation: Self-Management Strategies
The initial phase of care focuses on what you can do at home to calm symptoms and create an environment conducive to healing. This forms the foundation upon which other treatments are built.
The goal is to soothe, not strain. You are trying to calm irritated tissues, not push through the pain. This requires a balance of relative rest and gentle movement.
Key foundational strategies include:
- Activity Modification: This does not mean complete bed rest, which is rarely recommended. Instead, it involves thoughtfully avoiding activities that significantly worsen your pain—such as heavy lifting or prolonged sitting—while staying as active as you comfortably can.
- Heat or Cold Packs: A heat pack can help relax tight back muscles and improve blood flow. A cold pack is often better for reducing sharp pain and inflammation, particularly in the first 48 hours of an acute injury.
- Gentle Movement: Simple, non-straining movements can prevent stiffness and promote healing. This might include gentle pelvic tilts or bringing one knee to your chest at a time, but only if these movements do not provoke sharp leg pain. The guiding principle is to move without aggravating the primary symptom.
The Next Layer: Physiotherapy
If symptoms persist despite self-management, physiotherapy is the next logical step. A physiotherapist acts as a guide for your recovery, creating a structured program tailored to your specific diagnosis and physical capabilities.
A physiotherapist will assess your movement, strength, and symptom patterns to identify the root of the problem.
A typical physiotherapy plan for back and leg pain often includes:
- Targeted Stretching: To increase flexibility in tight muscles, such as the hamstrings or hip flexors, that may be contributing to mechanical stress on the back.
- Core Strengthening: To build muscular support for your spine, which can reduce the load on your discs and joints.
- Manual Therapy: Hands-on techniques used by the physiotherapist to gently mobilise stiff spinal joints and release deep muscle tension.
- Education: This is a vital component. You will learn about posture and body mechanics to help you move in ways that protect your back during daily activities.
In clinical experience, physiotherapy is a cornerstone for managing most types of back and leg pain. It provides the tools and knowledge for long-term success, aiming not only to relieve current pain but also to build resilience against future episodes.
Medical Interventions: When More Support is Needed
For some individuals, pain and inflammation are too severe to permit active participation in physiotherapy. In these cases, a GP or specialist may recommend medical treatments to control symptoms so that rehabilitation can proceed.
These are not first-line treatments but can be very helpful when conservative approaches are insufficient.
- Medications: Over-the-counter anti-inflammatory drugs like ibuprofen can help reduce inflammation. For nerve-related pain, a GP may prescribe specific medications designed to calm overactive nerve signals.
- Therapeutic Injections: If severe sciatica is caused by a clearly identified, inflamed nerve root, a targeted steroid injection can be effective. This delivers a potent anti-inflammatory directly to the source, often providing a window of pain relief that allows for meaningful engagement in physiotherapy.
Considering Surgical Options
Surgery is the final component of the treatment pathway and is appropriate for only a small percentage of people who meet specific criteria. It is rarely the first option and is generally considered only after a thorough trial of non-surgical treatments has failed to provide relief.
A discussion about surgery may arise if there is:
- Clear MRI evidence of nerve compression that directly corresponds with your symptoms.
- Progressive or worsening muscle weakness in your leg or foot.
- Severe, unremitting pain that has not responded to other treatments over a reasonable period.
The decision to proceed with surgery is a significant one, made collaboratively between you and your surgical team after carefully weighing the potential benefits and risks. The primary goal is typically to relieve pressure on the compressed nerve and, if necessary, to stabilise the spine.
What to Do Next
This article aimed to provide a calm, clear overview of why back and leg pain are often linked, how clinicians investigate these symptoms, and what the standard treatment paths involve.
However, lasting improvement is rarely achieved from a single article. Progress typically comes from following a consistent, structured plan that connects your symptoms to their likely cause and provides actionable steps. Moving from a state of confusion to one of clarity is a crucial first step.
From Learning to Doing
This information can serve as your foundation. When you understand the difference between radicular nerve pain and referred muscle pain, or you know why a physio is testing your reflexes, you are better equipped to participate in your own care.
This clarity is a powerful tool. It helps you have more productive conversations with your healthcare team, ask more targeted questions, and make informed decisions. You shift from being a passive recipient of care to an active partner in your recovery.
The turning point for many people occurs when they move from simply experiencing their pain to truly understanding it. This change in perspective is often key to managing it effectively.
Taking the Next Step
While articles like this are useful for building foundational understanding, they cannot provide a personalised, day-by-day plan. They explain the 'what' and 'why', but the 'how' often requires a more structured approach.
For readers wanting a more detailed and organised framework, we have created dedicated patient guides. They are designed for anyone who wishes to move beyond general advice and follow a clear path to managing their health. To explore a more methodical approach, you can view our collection of back patient guides.
Ultimately, the path you take from here is yours. The goal is that you can now move forward with more confidence and a clearer sense of direction.
At The Patients Guide, we create structured, easy-to-follow resources to help you connect the dots of your health. Browse our full library of guides at https://www.thepatientsguide.co.uk.
Also in News

Blood Test Results Time: Your UK Guide
Get precise blood test results time info for the UK in 2026. Understand NHS turnaround, common delays, how to check your results, and when to contact your GP.
Read More

Headache Quick Remedy: Immediate Relief Guide
Headache quick remedy - Find a headache quick remedy that works. Our guide helps you understand your headache and choose safe, effective action for immediate
Read More

Mouth Ulcers Treatment: A Clear Guide
A calm, clear guide to mouth ulcers treatment. Learn about causes, self-care, OTC options, when to see a doctor, and how to prevent recurring ulcers.
Read More